


Patient Resources: Embolisation
Definitions
Embolism refers to the migration of any substance not native to the blodd vessel coming from some other source.e.g tumor embolism wherein fragments of tumor invade the blodd vessel and carry on with the blood flow to occlude some other vessel. The process is called embolism, the material transported is called embolus (plural: emboli)
Embolization is a non-surgical, minimally-invasive procedure performed by an interventional radiologist and interventional neuroradiologists. It involves the selective occlusion of blood vessels by purposely introducing embolic material into the target blodd vessel.
The medical dictionary definition of embolisation is "therapeutic introduction of various substances into the circulation to occlude vessels, either to arrest or prevent hemorrhaging; to devitalize a structure, tumor, or organ by occluding its blood supply; or to reduce blood flow to an arteriovenous malformation."
Usage
Embolisation is used to treat a wide variety of conditions affecting different organs of the human body.







 Detachable balloon - Treats AVF and previosuly aneurysms, also to occlude blodd vessels in rare instances where the vessel need to be sacrificed e.g dissections, large aneurysms, carotid bloqout syndrome etc. These balloons are simply implanted in a target vessel, then filled with saline through a one-way valve. The blood stops and endothelium grows around the balloon until the vessel fibroses. Unfortunately, the balloon may be hypertonic relative to blood and hence rupture and fail, or it may be hypotonic and shrink, migrating to a new location.
Detachable balloon - Treats AVF and previosuly aneurysms, also to occlude blodd vessels in rare instances where the vessel need to be sacrificed e.g dissections, large aneurysms, carotid bloqout syndrome etc. These balloons are simply implanted in a target vessel, then filled with saline through a one-way valve. The blood stops and endothelium grows around the balloon until the vessel fibroses. Unfortunately, the balloon may be hypertonic relative to blood and hence rupture and fail, or it may be hypotonic and shrink, migrating to a new location.




Embolism refers to the migration of any substance not native to the blodd vessel coming from some other source.e.g tumor embolism wherein fragments of tumor invade the blodd vessel and carry on with the blood flow to occlude some other vessel. The process is called embolism, the material transported is called embolus (plural: emboli)
Embolization is a non-surgical, minimally-invasive procedure performed by an interventional radiologist and interventional neuroradiologists. It involves the selective occlusion of blood vessels by purposely introducing embolic material into the target blodd vessel.
The medical dictionary definition of embolisation is "therapeutic introduction of various substances into the circulation to occlude vessels, either to arrest or prevent hemorrhaging; to devitalize a structure, tumor, or organ by occluding its blood supply; or to reduce blood flow to an arteriovenous malformation."
Usage
Embolisation is used to treat a wide variety of conditions affecting different organs of the human body.
- Arteriovenous malformations (AVMs) and other vascular malformations
- Aneurysm
- Gastrointestinal bleeding
- Epistaxis
- Primary post-partum hemorrhage
- Surgical hemorrhage
- Post traumatic hemorrhage
- uterine fibroids
- Kidney lesions
- Liver lesions, typically hepatocellular carcinoma (HCC). Treated either by particle infarction or transcatheter arterial chemoembolization (TACE).
- Portal venous hypertension
Embolization may have 3 therapeutic goals:
- An adjunctive goal (eg, preoperative, adjunct to chemotherapy or radiation therapy)
- A curative goal (eg, definitive treatment such as that performed in cases of aneurysms, arteriovenous fistulae [AVFs], arteriovenous malformations [AVMs], and traumatic bleeding)
- A palliative goal (eg, relieving symptoms, such as those of a large AVM, which cannot be cured by using embolotherapy alone)
Embolization Materials And Substances
Materials used in embolization include coils, ethanol, sodium tetradecyl sulfate, cyanoacrylate, polyvinyl alcohol (PVA), microspheres, and gelatin sponge (Gelfoam), Onyx etc.
Coils
Coils can be grouped into microcoils and macrocoils. Macrocoils, also called Gianturco coils, were first introduced in 1975. Coils have the advantage of being precisely positioned under fluoroscopic control. Occlusion occurs as a result of coil-induced thrombosis rather than mechanical occlusion of the lumen by the coil. To increase the thrombogenic effect, Dacron wool tails are attached to coils. The coils are available in many sizes and may be delivered through commonly used angiographic catheters
Microcoils (platinum coils) can be delivered through venry thin and pliable microcatheters of less than 1 mm size. They can be particularly useful when superselective coil embolization is required. Microcoils are highly thrombogenic, radiopaque, and biocompatible. Again, the thrombogenic effect primarily results from the addition of silk or synthetic fibers, not from the coil.
Collateralization is a potential disadvantage of coil embolization, and it can result in the persistence of flow into the vascular territory of the vessel that was embolized with the coil. Additionally, when proximal occlusion occurs with coil embolization, repeat intervention via the same artery becomes difficult, if not impossible. Mechanically and electronically detachable coils are currently available.
In interventional neuroradiology practice, coils are used primarily for treating aneurysms and some times in large high flow AVM or fistulas.
Click here to see an example of coil embolisation (coiling) of an intracranial aneurysm
Ethanol
Ethanol (absolute alcohol) is one of the most commonly used liquid agent, though not in the neuro practice. Embolization with absolute alcohol has a direct toxic effect on the endothelium that activates the coagulation system and causes the microaggregation of red blood cells.
In the treatment of vascular malformations, ethanol has demonstrated its curative potential compared with the palliative effect seen with other embolic agents. Occlusion of the lumen occurs within minutes or days. Ethanol can be damaging if it reaches the capillary bed of any given tissue (eg, skin), and it usually causes significant soft-tissue swelling, which may subsequently cause compartment syndrome (nerve compression).
When absolute alcohol is mixed with a contrast medium and when small catheters are used, superselective vascular embolization can be safely performed under fluoroscopic guidance. Ethiodized oil (Ethiodol), an oily contrast medium, is used most commonly.
If large amounts of absolute alcohol enter the systemic circulation, toxic effects can occur. These include central nervous system (CNS) depression, hemolysis, and cardiac arrest. Slow, careful injections by using balloon occlusion arterial catheters for delivery and by applying manual compression on the draining veins (or tourniquet control) or balloon occlusion of the draining system may decrease alcohol washout from the lesion and reduce acute systemic toxicity. Ethanol 1 mg/kg is the maximum amount that can be injected during a single session.
Sodium tetradecyl sulfate
Sodium tetradecyl sulfate (Sotradecol) is another sclerosant. This contains 2% benzyl alcohol and is commonly used for AVMs and varices. Use of this agent is less painful for the patient, and it is considered to be less toxic then absolute alcohol. Therefore, some lesions can be treated without general anesthesia.
Sodium tetradecyl sulfate can be used as a sclerosant in various concentrations (1-3%); however, manufacture of this agent has been discontinued in the United States. This author has begun using ethanolamine oleate instead of sodium tetradecyl, with the same indications.
Cyanoacrylate
Cyanoacrylate, or N- -butyl-2-cyanoacrylate (NBCA) is a rapidly hardening liquid adhesive often referred to as glue. The substance hardens (polymerizes) immediately on contact with blood or other ionic fluid. Polymerization results in an exothermic reaction that destroys the vessel wall.
Penetration of the capillary bed causes severe tissue injury. Because of the rapid polymerization, coaxial catheterization, precise positioning of the delivery catheter, and considerable skill are required for NBCA embolization. When a suitable location is reached by using a microcatheter, the catheter is flushed with 5% dextrose to clear it of any blood or contrast medium.
Under real-time fluoroscopic control, a mixture of NBCA and oily contrast medium is delivered. As soon as a cast of the vascular tree is seen fluoroscopically, the delivery microcatheter is quickly removed so that the catheter tip does not adhere to the vessel. Again, the catheter is flushed quickly with 50% dextrose so that it can be reused during the same procedure.
A foreign-body inflammatory reaction is the primary disadvantage of the use of this embolic material.
This is the most commonly used material in intracranial and spinal AVM and dural AVF embolisation.
Polyvinyl alcohol
PVA is obtained by the reticulation of PVA (Ivalon) with formaldehyde. PVA is available as particles with a large range of sizes. For sizes as large as 710 μ m, a microcatheter can be used as a delivery catheter.
Successful PVA-particle embolization depends on the formation of a thrombus in which a large proportion of the embolized vessel is filled with thrombus rather than PVA particles. Histologically, this agent causes intraluminal thrombosis associated with an inflammatory reaction, with subsequent organization of the thrombus. PVA is considered a permanent embolic agent because of the low frequency of recanalization of the embolized vessels. PVA is not absorbable, and it likely produces permanent occlusion.
PVA is usually administered in a mixture of contrast medium and isotonic sodium chloride solution under fluoroscopic guidance. Aggregation of PVA particles can be minimized by using dilute contrast medium in a matched-density suspension; for example, Omnipaque and sodium chloride solution can be used in a ratio of 1:0.4 for contour particle suspension. PVA particles have a tendency to aggregate within the vessel once administered, potentially leading to an occlusion that is more proximal than intended. Diluted mixtures advance more distally, whereas concentrated mixtures cause more proximal occlusions.
PVA particle embolisation is primarily used for tumor embolisation and sometimes in AVms and dural AVFs.
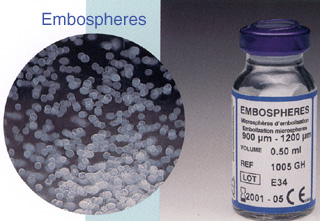
Tris-acryl gelatin microspheres
Microspheres (Embosphere; Biosphere Medical, Rockland, Mass) are biocompatible, hydrophilic, nonresorbable, and precisely calibrated particles produced from an acrylic polymer and impregnated with porcine gelatin. Microspheres are available in sizes of 40-1200 µm, and they are supplied in apyrogenic sterile sodium chloride solution.
To provide the desired clinical outcome, appropriately sized microspheres and delivery catheters must be chosen to best match the size of the target vessel. For example, when AVMs are being embolized, choose a particle size that occludes the nidus without passing into the systemic circulation. These particles typically do not aggregate, and this is a distinct advantage of microspheres compared with PVA particles.
Microspheres can tolerate temporary compression of 20-30% to facilitate their passage through the delivery catheter. When a coaxial technique is used, a 2.5-3.0F microcatheter allows the passage of microspheres as large as 700 µm for embolization.
Because microspheres are not radiopaque, contrast enhancement must be used to monitor embolization under fluoroscopic guidance. Microspheres are considered permanent embolic particles.
Gelfoam
Gelfoam is a sterile gelatin sponge intended for application to bleeding surfaces for hemostasis or for use as a temporary intravascular embolic material. It is a water-insoluble, off-white, nonelastic, porous, and pliable material. Gelfoam may be cut without fraying, and it can absorb and hold many times its weight in blood and other fluids.
Gelfoam is usually absorbed completely (depending on the amount used, degree of saturation with blood, and site at which it is used), with little tissue reaction. When used as an embolic material, the vessel recanalizes within a few weeks. Gelfoam is supplied in a sterile envelope enclosed in an outer peelable envelope. It is available in sizes from 12 mm to 6 cm.
Click here to see an example of balloon embolisation of a carotico-cavernous fistula (CCF)
Other materials
Other less commonly or previously used materials include balloons, microfibrillar collagen (Avitene), autologous materials, ethylene vinyl alcohol, alginates, phosphoryl choline, sodium morrhuate, hot contrast material, and 50% dextrose.
ONYX
ONYX is a patented liquid embolic material from ev3 company, a relatively new entrant in the field of interventional neuroradiology and has provided an exciting new way treat complex AVMs and dural AVFs which otherwise were difficult to treat.
ONYX is a patented liquid embolic material from ev3 company, a relatively new entrant in the field of interventional neuroradiology and has provided an exciting new way treat complex AVMs and dural AVFs which otherwise were difficult to treat.
Onyx® LES
Onyx® is a non-adhesive liquid embolic agent used for the pre-surgical embolization of brain Arteriovenous malformations (bAVM).
- Onyx is comprised of EVOH (ethylene vinyl alcohol) copolymer dissolved in DMSO (dimethyl sulfoxide), and suspended micronized tantalum powder to provide contrast for visualization under fluoroscopy.
- The Onyx Liquid Embolic System (LES) consists of a 1.5 ml vial of Onyx, a 1.5 ml vial of DMSO, and three 1 ml Onyx delivery syringes.
- A DMSO compatible delivery micro catheter that is indicated for use in the neuro vasculature (e.g. Marathon™, Rebar® or UltraFlow™ HPC catheters) is used to access the embolization site.
- Onyx is available in two product formulations, Onyx 18 (6% EVOH) and Onyx 34 (8% EVOH).
Onyx® HD-500
Onyx® 500 is a non-adhesive liquid embolic agent used for the embolization of brain aneurysms.- Onyx HD500 is comprised of 20% EVOH (ethylene vinyl alcohol) copolymer dissolved in DMSO (dimethyl sulfoxide), and suspended micronized tantalum powder to provide contrast for visualization under fluoroscopy.
- Onyx HD500 (20% EVOH) is an HDE device for the treatment of intracranial, saccular, sidewall aneurysms that present with a wide neck (≥ 4mm) or with a dome-to-neck ratio < 2 that are not amenable to treatment with surgical clipping.
- Onyx HD500 can also be used in adjunctive therapy with Axium coils and stents.
Procedure
The procedure is a minimally invasive alternative to surgery. The purpose of embolization is to prevent blood flow to an area of the body, which effectively can shrink a tumour or block an aneurysm etc.
The procedure is carried out as an endovascular procedure by a consultant radiologist in an interventional suite. It is common for most patients to have the treatment carried out with little or no sedation, although this depends largely on the organ to be embolized. Patients who undergo cerebral or spinal embolization are usually given a general anesthetic.
Access to the organ in question is acquired by means of a guidewire and catheter(s). Depending on the organ this can be very difficult and time consuming. The position of the correct artery or vein supplying the pathology in question is located by digital subtraction angiography (DSA). These images are then used as a map for the radiologist to gain access to the correct vessel by selecting an appropriate catheter and or wire, depending on the 'shape' of the surrounding anatomy.
Sometimes, direct percutaneous access to the lesion adn organ can be made e.g in liver, face etc. In such cases, multiple fine needles and inserted and placed inside the lesions and the embolic material injected directly.
Advantages
- Minimally invasive
- No scarring
- Minimal risk of infection
- No or rare use of general anesthetic
- Faster recovery time
- High success rate compared to other procedures
- Preserves fertility and anatomical integrity
Disadvantages
- User dependent success rate
- Risk of emboli reaching healthy tissue
- Not suitable for everyone
- Recurrence more likely
Tags: Patient Resources
Subscribe to:
Post Comments (Atom)








Share your views...
0 Respones to "Patient Resources: Embolisation"
Post a Comment